Disease Overview
The vertebrae of the backbone are cushioned by intervertebral discs that act as shock absorbers and allow frictionless movement of your back. It is made up of a soft gel-like center called the nucleus pulposus that is surrounded by a tough outer ring of annulus fibrosus. A herniated disc is a condition in which the nucleus pulposus bulges out through the damaged or broken annulus fibrosus. This puts pressure on the neural structures, such as nerve roots and/or the spinal cord. Besides, bony outgrowths, also known as bone spurs or bone osteophytes, are formed due to the accumulation of calcium in the spine joints. The pressure induced by a herniated disc or bone spur on nerve roots, ligaments or the spinal cord may cause pain in the neck and/or arms, numbness or weakness in the arms, forearms or fingers, and lack of coordination.
As most nerves to the body (e.g., arms, chest, abdomen, and legs) pass through the neck region from the brain, pressure on the spinal cord in the neck region (cervical spine) can be very problematic.
What is Anterior Cervical Discectomy and Fusion?
Anterior cervical discectomy with fusion is an operative procedure to relieve compression or pressure on nerve roots and/or the spinal cord due to a herniated disc or bone spur in the neck. The vertebra is approached from the from (anterior) of your neck.
Indications for Anterior Cervical Discectomy and Fusion
Anterior cervical discectomy with fusion is recommended only after non-surgical treatment approaches fail. Before recommending surgery, your surgeon considers several factors such as your health condition, age, lifestyle and anticipated level of activity following surgery.
Anterior Cervical Discectomy and Fusion Procedure
- Your surgeon makes a small incision in the front side of the neck and locates the source of neural compression (pressure zone).
- Then, the intervertebral disc that is compressing the nerve root will be removed partially or completely along with any bony material that is compressing or putting pressure on the nerves and producing pain.
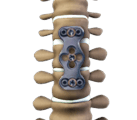
- Spinal fusion implies placing a bone graft between the two affected vertebral bodies to encourage bone growth between the vertebrae.
- The bone graft acts as a medium for binding the two vertebral bones and grows as a single vertebra to stabilize the spine.
- It also helps to maintain the normal disc height. In certain instances, metal plates or pins may be used for providing support and stability and enabling the fusion of the vertebrae.
Postoperative Instructions Anterior Cervical Discectomy and Fusion
A specific postoperative recovery/exercise plan will be offered by your physician to help you return to normal activity at the earliest possible. The duration of hospital stay depends on this treatment plan. You will be able to wake up and walk by the end of the first day after the surgery and resume your work within 3-6 weeks, depending on your body’s healing status and the type of work/activity that you plan to resume.
Risks or Complications of Anterior Cervical Discectomy and Fusion
In addition to the anesthetic complications, spinal surgery is associated with some potential risks such as infection, blood loss, blood clots, nerve damage, and bowel and bladder problems. Failure to fuse the vertebral bones with the bone graft (fusion failure) is an important complication of spinal fusion, which usually requires additional surgery.
Related Topics
Cervical
- Artificial Cervical Disc Replacement
- Cervical Disc Replacement
- Cervical Bracing
- Cervical Foraminotomy
- Cervical Laminectomy
- Cervical Laminoplasty
- Cervical Spine Fusion
- Posterior Cervical Fusion
- Posterior Cervical Decompression
- Anterior Cervical Discectomy and Fusion
Lumbar
- Lumbar Decompression
- Lumbar Discectomy
- Lumbar Endoscopic Discectomy
- Lumbar Epidurals
- Lumbar Foraminotomy
- Lumbar Laminectomy
- Lower Back (Lumbar) Surgery
- Lumbar Interbody Fusion
- Lumbar Microdiscectomy
- Lumbar Medial Branch Block
- Lumbar Spinal Fusion
- Lumbar Spinal Bracing
- Posterior Lumbar Fusion
- Posterior Lumbar Interbody Fusion
- Transforaminal Lumbar Interbody Fusion (TLIF)
Thoracic
- Thoracic Discectomy
- Thoracic Laminectomy
- Thoracic Spine Decompression
- Thoracic Spine Fracture Repair Surgery
- Thoracic Spine Trauma Surgery
- Thoracic Vertebroplasty
- Posterior Thoracic Fusion
Others
- Minimally Invasive Spine Surgery
- Image-Guided Spine Surgery
- Revision Spinal Surgery
- Robotic Spine Surgery
- Complex Spine Surgery
- Spinal Fusion
- Spinal Decompression
- Spinal Nerve Blocks
- Epidural Steroid Injections
- Transforaminal Epidural Steroid Injection
- Foraminoplasty
- Microdiscectomy
- Laminectomy
- Vertebroplasty
- Radiofrequency Ablation
- Outpatient Spine Surgery
- Spinal Infection Stabilisation
- Spine Osteotomy
- Spinal Tumor Surgery
- Spinal Cord Stimulator
- Posterior Scoliosis Surgery
- Removal of Facet Joint Cyst
- Non-Surgical Treatment for Disc Disease
- Physical Therapy for the Spine


